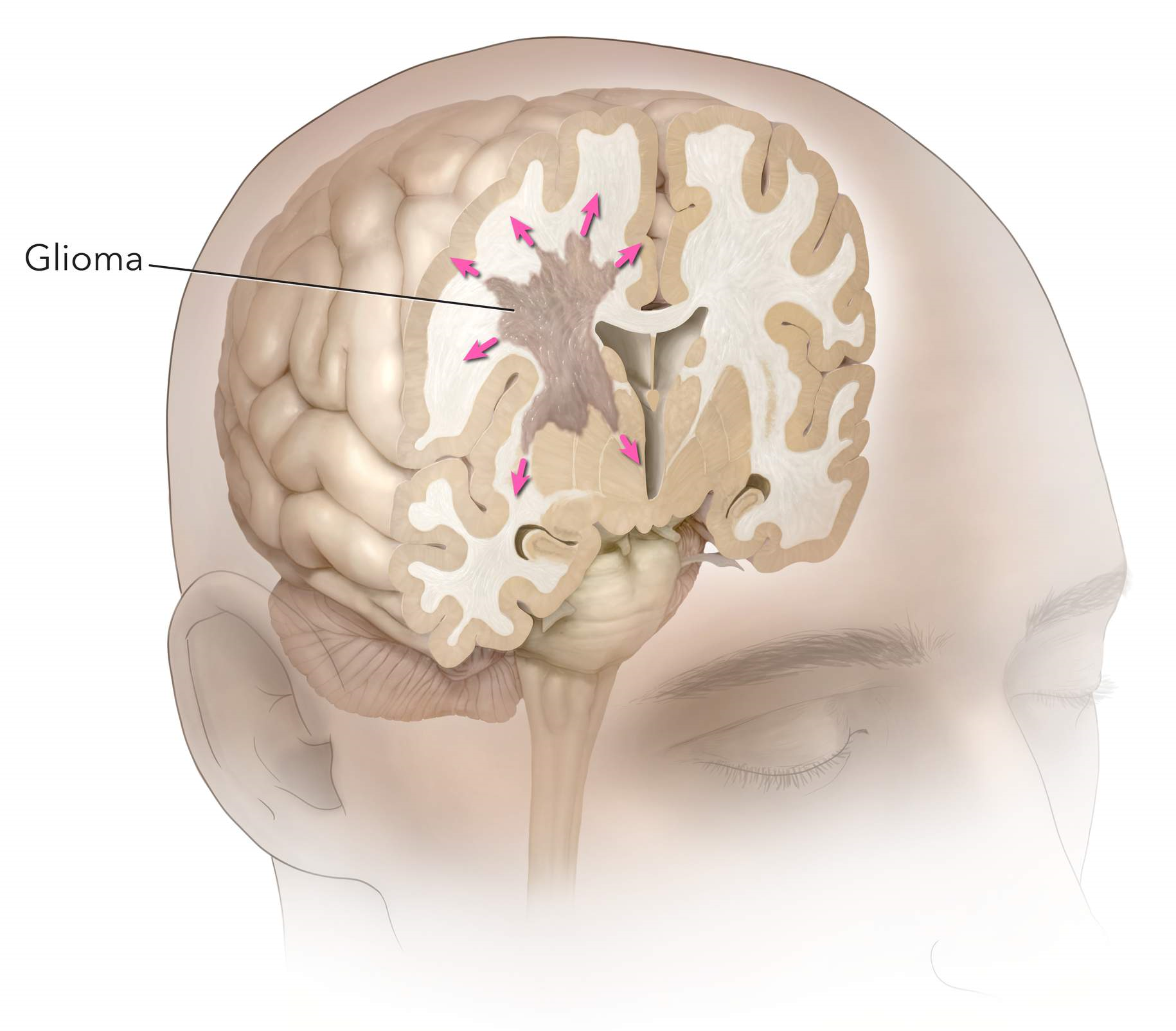
“Glioma” is a term used to describe any tumour that arises from the supportive “glial” tissue of the brain. This tissue helps in proper functioning of the neurons.
“Glioma” is a term used to describe any tumour that arises from the supportive “glial” tissue of the brain. This tissue helps in proper functioning of the neurons.
The three main types of glial cells that can produce tumours are: astrocyte, ependymal and oligodendrocyte which produces astrocytomas, ependymomas and oligodendrogliomas, respectively. And, the tumour that displays a mixture of these cells are called mixed gliomas.
Each of these cerebral tumour types, accounting for nearly 45 percent of cancers that begin in brain cells, can be assigned a grade; either low or high, with high grade being more malignant and aggressive.
Astrocytomas: These tumours are graded on a scale from I to IV. Low-grade astrocytomas are usually localised and grow slowly whereas high-grade astrocytomas grow at a rapid pace and require aggressive treatment.
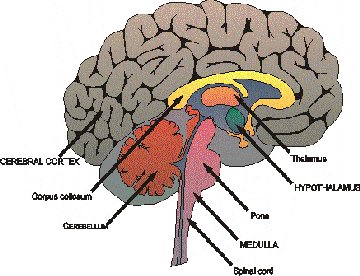
Astrocytomas can appear in various parts of the brain and nervous system, including the cerebellum, the cerebrum, central areas of the brain, the brainstem, and the spinal cord. Most of these tumours diagnosed in children are low grade while the ones found in adults are high grade.
* Pilocytic Astrocytoma, also called Juvenile Pilocytic Astrocytoma, are grade I astrocytomas. These typically do not spread and are considered the “most benign” (noncancerous) of all the astrocytomas. Two other, less well known grade I astrocytomas are Cerebellar Astrocytoma and Desmoplastic Infantile Astrocytoma.
* Diffuse Astrocytoma are also called as Low-Grade or Astrocytoma Grade II tumours. The common types are Fibrillary, Gemistocytic, Protoplasmic Astrocytoma. These types tend to invade surrounding tissue and grow at a relatively slow pace.
* Anaplastic Astrocytoma is a grade III tumour. These rare tumours require comparatively more aggressive treatment than grade I and II.
* Astrocytoma Grade IV are also called Glioblastoma tumours. These are further subdivided into primary and secondary types. Primary tumours are common and more aggressive while the secondary tumours are the ones that originate as a lower-grade tumour but these later evolve into a grade IV.
* Subependymal Giant Cell Astrocytoma are ventricular tumours associated with tuberous sclerosis.
Ependymomas: These arise from the ependymal cells that are found lining certain areas of the brain and spinal column. These cells help in repairing the damaged nerve tissues.
* Subependymomas (grade I): These are the slow-growing tumours that appear near a ventricle.
* Myxopapillary Ependymomas (grade I): These too belong to the slow-growing tumours’ category and are commonly found in the lower part of spinal column.
* Ependymomas (grade II): These are the most common of the ependymal tumours. This type can be further subdivided into Cellular Ependymomas, Papillary Ependymomas, Clear Cell Ependymomas, and Tancytic Ependymomas. These cells are located along, within, or next to the ventricular system.
* Anaplastic Ependymomas (grade III): These belong to the category of faster-growing tumours and are commonly found in the brain. Like Astrocytomas, Ependymomas too are commonly seen in children and young adults.
Oligodendrogliomas: These tumours form in oligodendrocyte cells, which produce a fatty substance called myelin that protect our nerves. They can be low-grade (grade II) or high-grade (grade III, or anaplastic) tumours found anywhere within the cerebral hemisphere of the brain, although the frontal and temporal lobes are the most common locations.
Common in adults, these tumours may move to other parts of the brain or spinal cord.
Mixed Glioma: These tumours usually contain more than one type of cell, most often astrocytes and oligodendrocytes. Occasionally, ependymal cells are also found. The behavior of a mixed glioma appears to depend on the grade of the tumour.
Brain Stem Glioma: These are rare tumours located in brain stem. Treatment may be in the form of surgery and/or radiation.
Optic Glioma: These tumours may involve any part of the optic pathway, and have the potential to spread. Most of these tumours occur in children under the age of 10 years. Infact, 20 percent of children with neurofibromatosis (NF-1) will develop an optic glioma. These gliomas are typically grade I, Pilocytic Astrocytomas.
The early signs of a glioma brain tumour may depend on the tumour type. But when diagnosed with either of these symptoms it is recommended to proceed with special neurological investigations. However, the common symptoms may include:
*Rise in intracranial pressure
*Epilepsy
*Mental/behavioral changes
*Abnormal neurological signs like sensory loss, squint, etc.
*Headaches
*Nausea and vomiting
*Changes in speech
*Walking difficulties
*Vision changes and abnormal eye movements
Diagnostic tests used to detect glioma include:
* Physical examination
* Medical history
* CT scan
* MRI scan
* Biopsy
The treatment for glioma brain tumour will depend on factors like the grade of the brain tumour, patient’s age and health history, how much tumour can be removed, its location and size, etc.
Surgery is usually the first line of treatment to remove or decompress the tumour and to make the diagnosis.
However, patients diagnosed with glioma tumour often receive a combination of different types of treatments like chemotherapy, radiation therapy, and surgery for the best chance of recovery and survival.
A craniotomy is a procedure in which a hole is cut into the skull in order to provide access to the brain. This allows a biopsy of the glioma and the opportunity to remove the tumour at the same time. After the operation is finished, the bone is replaced, and the muscle and skin are stitched.
The surgery is often followed by radiotherapy or chemotherapy.
The radiotherapy will not cure the cancer but aims to try to control the tumor for as long as possible. The aim of the treatment is to slow down the tumour growth.
It uses a combination of powerful medications that helps to destroy cancer cells. Unfortunately, chemotherapy medications tend to affect healthy cells in the body which may cause side effects such as hair loss and vomiting, etc.
Copyright © 2020. All Rights Reserved.
Designed and Developed by Easy Solution 360